A healthy baby who was laughing and playing suddenly draws up their legs and screams. The crying stops for a few minutes. Then it starts again — just as suddenly and just as violently. In between these episodes, your baby looks pale and exhausted. Later, you notice something alarming in the nappy: jelly-like red and brown mucus, with almost no normal stool.
This pattern — sudden colicky pain in episodes, with blood and mucus in the stool — is the classic warning sign of intussusception. It is one of the most important bowel emergencies in young children, and it needs to be treated within hours.
The good news: when caught in time, intussusception can very often be treated without surgery.
What Is Intussusception?
The word sounds complicated, but the picture is simple.
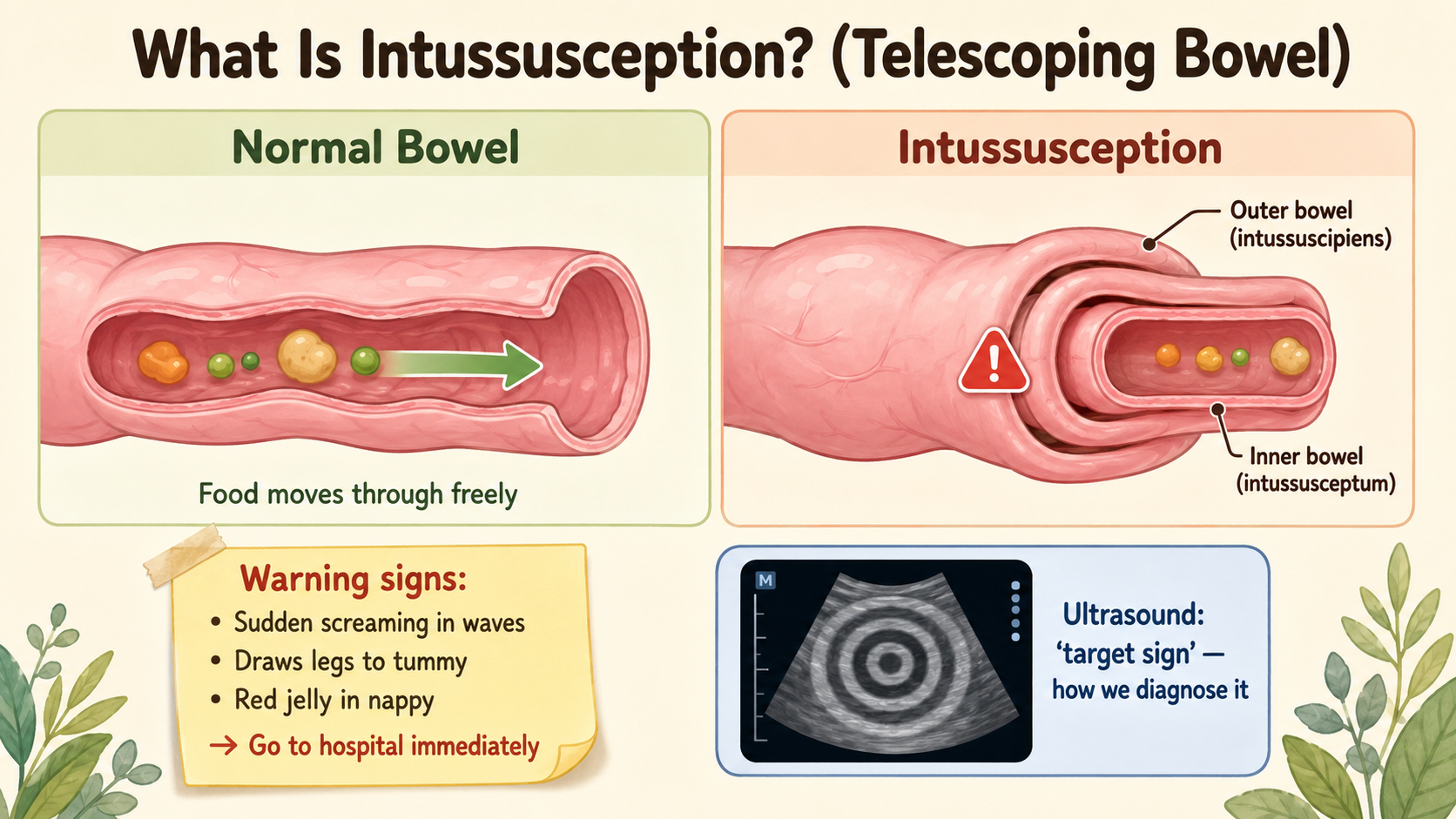
The small intestine is a long, hollow tube. Intussusception happens when one section of this tube telescopes into the section next to it — like a sock being pushed inside-out. The inner segment gets stuck inside the outer one.
When this happens:
- The bowel is blocked — nothing can pass through
- The blood supply to the trapped inner segment is compressed
- The bowel begins to swell and, if not released, begins to die
This is why it must be treated urgently.
Who Gets It?
Intussusception is primarily a condition of young children. The peak age is between 3 months and 3 years, with the highest concentration of cases in babies between 6 and 9 months of age — when weaning begins and the lymph nodes in the bowel wall are most active.
About 75% of all cases occur in the first 2 years of life, and 90% occur before age 3. It is slightly more common in boys.
In infants and toddlers under 2 years, it almost always starts spontaneously — no cause can be found. In older children (over 5 years), intussusception is more often caused by something inside the bowel acting as a “lead point” — a Meckel’s diverticulum, an intestinal polyp, or rarely a lymphoma. Up to 60% of cases in older children have an identifiable cause.
What Are the Warning Signs?
The classic triad of intussusception is:
1. Sudden, severe, colicky abdominal pain — in episodes. The baby screams and draws up the knees, then goes quiet and limp for a few minutes, then screams again. The episodes come in waves because the bowel is intermittently squeezing against the blockage. Parents often describe the child looking well between episodes — which is exactly right.
2. Vomiting. Initially non-bilious (clear or milky). If the obstruction has progressed, the vomit may become yellow or green — a sign that the blockage is complete.
3. “Red currant jelly” stool. Blood and mucus are shed from the damaged, congested bowel lining and come out together as dark red, jelly-like material in the nappy. This is a late sign — it means the bowel is being injured. Do not wait to see this before going to hospital.
An experienced examiner may also feel a sausage-shaped mass in the upper abdomen. There is often an odd feeling of emptiness in the lower right part of the belly — the bowel that is usually there has telescoped away.
All three signs are present together in only about 25 to 30% of children. Do not wait for the full picture. If a young child has sudden, episodic, inconsolable crying with vomiting — even without blood in the stool — go to a hospital.
How Is It Diagnosed?
An ultrasound of the abdomen is the best and safest way to diagnose intussusception. It is fast, involves no radiation, and is accurate close to 100%.
What the radiologist sees on ultrasound:
- A “target” or “doughnut” sign — layers of bowel-within-bowel appearing as concentric rings, seen from the front
- A “pseudokidney” sign — an oval, layered mass when seen from the side
The diagnosis is usually confirmed within minutes. No X-ray or CT scan is needed for a straightforward case.
How Is It Treated?
In most cases — no surgery.
If your child is brought in within the first 12 to 24 hours, is not very unwell, and there are no signs of bowel perforation, the standard first treatment is an air or fluid enema:
A small tube is passed into the back passage. Air (or a special fluid) is gently pumped in under pressure and guided by X-ray. This pressure pushes the telescoped segment backwards — like reversing the sock — and releases the blockage.
This procedure works in 70 to 90% of cases. In experienced centres, success rates approach 95%.
When it works, it is complete: the blockage opens up, the child passes stool normally within hours, and is usually home the same day.
When is surgery needed?
Surgery is required when:
- The bowel has already perforated (a hole has formed) — there are signs of peritonitis or free air on imaging
- The child is in shock, sepsis, or very unwell — the enema would be unsafe
- The enema has been tried and has not succeeded
- An older child has a lead point (like a Meckel’s diverticulum) that caused the intussusception — the lead point itself needs to be removed
During surgery, the telescoped bowel is gently reduced by hand. If the bowel is already dead, the damaged segment is removed and the two healthy ends are joined.
Will It Come Back?
After a successful enema reduction, intussusception comes back in approximately 10% of children. Most recurrences happen in the first 24–48 hours, which is why we keep children for observation. A second enema is usually successful. After two or three recurrences, surgical evaluation may be recommended to look for a lead point.
What Every Parent Must Know
Intussusception is a time-sensitive emergency. The longer the bowel remains telescoped:
- The more it swells and becomes damaged
- The less likely the enema is to work
- The more likely surgery becomes
Go to a hospital immediately if your child (under 3 years old):
- Has sudden, severe, episodic crying where they draw up their legs
- Vomits and looks pale between episodes of pain
- Passes blood or jelly-like material in the stool
- Was well until an hour ago and is now screaming inconsolably
Do not wait overnight. Do not give pain medicine and watch. This is one of the conditions where every hour matters.
When to See a Pediatric Surgeon
Any child with suspected intussusception needs assessment at a paediatric surgical centre with ultrasound capability and the ability to perform an enema reduction. If your child has been assessed at a local hospital and the ultrasound is inconclusive, ask for a referral to a centre with paediatric surgical expertise.
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He manages children with intussusception and other bowel emergencies from across Chhattisgarh and central India. For urgent cases, go directly to the nearest hospital with paediatric surgical facilities.
Related reading:
- Baby Not Passing Stool Since Birth? It Could Be Hirschsprung Disease
- Appendicitis in Children: When Stomach Pain Needs Surgery
- Constipation in Children: Causes, Treatment & When to See a Pediatric Surgeon
📋 This article is part of Dr. Motiwala’s Pediatric General & Abdominal Surgery in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
- Appendicitis in children
- Pyloric stenosis (forceful vomiting in babies)
- Testicular torsion (sudden testicle pain)
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child. In an emergency, go to the nearest hospital immediately.
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); DK Gupta Pediatric Surgery Vol 1.