You go for a routine pregnancy scan and the report says your baby’s kidney looks “swollen,” “dilated,” or has “hydronephrosis.” It is one of the most common findings on antenatal ultrasound — and one of the most frightening things to read when it is your baby. The reassuring headline first: in most babies, this settles on its own and never causes a problem. But a small number of cases point to something that genuinely needs treatment, so it should be checked properly, not ignored. Here is what it means.
What “Hydronephrosis” Actually Means
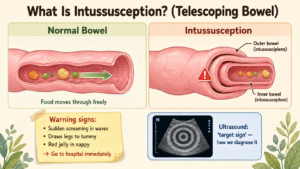
Each kidney makes urine, which collects in a funnel-shaped space (the renal pelvis), then drains down a narrow tube (the ureter) into the bladder. Hydronephrosis simply means that funnel is swollen with urine — either because urine is draining a little slowly, or because it is backing up. On the scan it shows as a dark, fluid-filled space in the middle of the kidney.
Doctors grade how much the kidney is dilated, often using the Society for Fetal Urology (SFU) scale from Grade 1 (mild) to Grade 4 (severe), where the higher grades show ballooned calyces and thinning of the kidney tissue. The grade matters, because mild dilation behaves very differently from severe dilation.
The Reassuring Part — Most Cases Settle
This is the number worth holding on to: between about 50% and 80% of hydronephrosis picked up before birth resolves on its own, either before delivery or in the months afterwards. In many babies it is simply an immature, slightly sluggish drainage system that matures and catches up. That is precisely why the biggest mistake in this condition is over-treating — rushing to surgery on a kidney that would have settled by itself. The finding is common and usually not dangerous; it earns a proper check-up, not a panic.
What Can Cause It
Antenatal hydronephrosis is a sign, not a single disease, and it has several possible causes:
- Transient (physiological) dilation — the commonest cause, and the one that simply resolves.
- PUJ (pelvi-ureteric junction) obstruction — a narrowing where the funnel meets the ureter. It is the commonest obstructive cause, affects boys about twice as often as girls, and is more often on the left.
- Vesicoureteric reflux (VUR) — urine flowing backwards from the bladder up towards the kidney.
- A blockage lower down — for example a narrowing where the ureter meets the bladder (an obstructed megaureter).
- Posterior urethral valves (PUV) — a blockage at the bladder outlet. This one occurs only in boys and is the serious cause to catch early (see below).
The One Pattern That Needs Urgent Attention
There is a specific picture on the antenatal scan that changes everything: a boy with BOTH kidneys dilated, a large thick-walled bladder that will not empty (the “keyhole sign”), and reduced fluid around the baby (low amniotic fluid). This combination strongly suggests posterior urethral valves — the commonest cause of bladder-outlet blockage in newborn boys.
PUV matters for two honest reasons. Before birth, low amniotic fluid can hold back the baby’s lung development. And even after the blockage is treated, the back-pressure can leave lasting kidney damage: roughly 20% to 50% of boys with posterior urethral valves eventually develop kidney failure, sometimes not until adolescence — so these boys need lifelong kidney and urology follow-up. If this pattern is seen, delivery should be planned at a centre with newborn surgical and urology care ready.
What Happens After Birth
For most babies the plan is calm and staged:
- A repeat ultrasound after birth confirms whether the dilation is still present and grades it. Mild cases are simply watched with scans over time.
- A bladder X-ray test (a micturating cystourethrogram, MCU/VCUG) is added if both kidneys are involved, the dilation is significant, or valves or reflux are suspected — especially in a boy, to rule out PUV.
- A MAG-3 diuretic renogram, usually around 3–4 weeks of age, measures how well each kidney works and whether it is draining freely.
- Preventive antibiotics are sometimes given while a kidney is being watched, to reduce the chance of a urine infection.
Does It Need Surgery?
Usually not. Most babies are simply monitored, and the dilation improves. Surgery is reserved for clear reasons — for a PUJ obstruction, an operation called a pyeloplasty (which rebuilds the narrowed junction) is considered mainly when the kidney’s share of function drops below about 40%, when function falls on repeat scans, or when the hydronephrosis is clearly getting worse. Posterior urethral valves are treated in the newborn period by removing the obstructing valve.
The honest picture: for straightforward PUJ obstruction, results after pyeloplasty are very good. For posterior urethral valves, treatment protects the kidneys but does not undo damage already done before birth — which is exactly why early recognition and long-term follow-up matter so much.
When to See a Pediatric Surgeon
If an antenatal scan shows hydronephrosis, arrange a review with a paediatric surgeon or paediatric urologist so the after-birth checks are planned in advance. It becomes urgent when the scan shows a boy with both kidneys dilated and a full, thick bladder — that baby should be delivered and reviewed where newborn urological care is available.
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He counsels parents on antenatally detected hydronephrosis and manages children with PUJ obstruction, reflux and posterior urethral valves from across Chhattisgarh and central India. If your pregnancy scan mentioned a swollen kidney, it is worth a calm, planned review — not a panic.
Related conditions parents also read
- My child keeps getting urine infections — is there a hidden kidney problem?
- Undescended testis in baby boys
- Hypospadias in newborn boys
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child.
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); Kelalis-King-Belman Clinical Pediatric Urology.