For most parents, the first time they hear the word “hypospadias” is in the newborn nursery — or from a grandmother who has noticed the baby’s urine goes downwards, not forwards. The mother almost always feels guilt: “Did I do something wrong in pregnancy?”
The honest answer is no. Hypospadias is one of the most common birth differences in boys, it is not caused by anything the mother did, and with the right surgery the long-term result is excellent. Here are the key points every parent should know.
What Is Hypospadias?
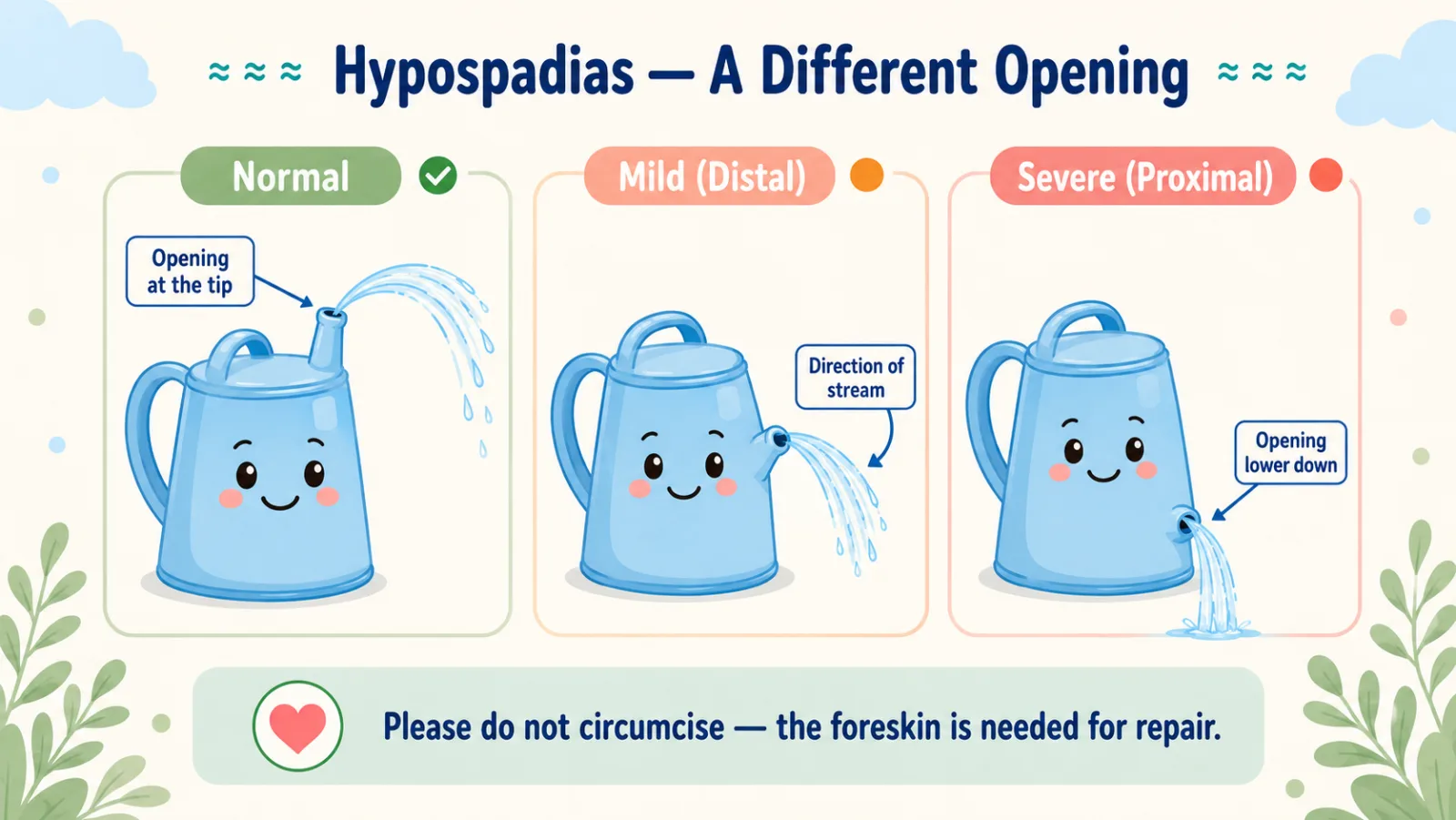
In a normally formed penis, the urinary opening is at the tip of the head, the foreskin fully covers it, and the shaft is straight.
In a boy with hypospadias, three things happen together:
- The urinary opening sits on the underside of the penis, anywhere from just below the tip down to the scrotum.
- The foreskin is incomplete on the underside — forming a “hood” only on the top.
- The penis often has a downward curve during erection, called chordee.
It is a developmental event in early pregnancy — not hereditary in most cases, and not something a mother causes.
How Common Is It?
About 1 in every 200 to 300 baby boys is born with hypospadias. It is far more common than most parents realise — and the outcome with modern surgery is very good.
The One Rule Every Parent Must Know: Do Not Circumcise
I cannot stress this enough.
A boy with hypospadias must NOT be circumcised in the newborn period — for any reason — until a pediatric urologist has examined him.
Why? Because the foreskin is the single most valuable piece of tissue the surgeon will use to rebuild the missing part of the urethra and cover the underside of the penis. Once it is removed, the repair becomes much harder and the result less good.
If your pediatrician spots hypospadias in the nursery — postpone any planned circumcision and get a pediatric urology opinion first.
When Is Surgery Done?
The right window is between 6 and 18 months of age, with most pediatric urologists preferring 6 to 12 months. The reasons:
- The baby is still in diapers — post-operative care is easy
- The child is mostly immobile and will not pull at dressings
- It is before the child develops genital awareness — so no psychological impact
There is no advantage to operating in the first weeks, and no advantage to waiting until school age.
What Does the Surgery Involve?
The exact technique depends on where the opening sits and how much curve the penis has. In most cases:
- It is a single-stage day-care or short-stay operation under general anaesthesia
- The opening is brought to the tip, the curve is straightened, and the foreskin tissue is used to rebuild the missing part
- A small catheter or stent is left in for a few days
- Most children recover comfortably at home, with a follow-up visit in a week
For more severe forms (where the opening is near the scrotum), the repair may be planned in two stages, six months apart. We will go through the exact plan with you at the first visit.
What About Complications?
Honest disclosure matters. Overall, complications happen in about 10 to 20% of operations, and the risk goes up with the severity of the original problem.
The commonest is a tiny leak between the new urethra and the skin (called a fistula) — under 5% in mild cases, higher in severe ones. Most complications are correctable with a small second procedure.
We plan for one operation — but a small chance of needing a touch-up later is part of the honest contract.
The Long-Term Outlook — The Reassuring Part
With modern repair done in expert hands:
- The new urethra grows with the child through puberty
- The urinary stream becomes forward-directed — your son will stand and urinate normally
- Adult sexual function and fertility are preserved
- The scar is hidden along the natural midline of the penis
Most adult men who had hypospadias repair as infants lead completely normal sexual and reproductive lives.
Common Questions Parents Ask
Did I cause this during pregnancy? No. Please let go of this guilt — it is not your fault.
Will my child urinate normally? After repair, yes — standing, with a forward stream.
Will sexual function be normal as an adult? In the vast majority of cases, yes.
Is it hereditary? A familial tendency exists: the risk in brothers of affected boys is approximately 6–21%, and in fathers of affected boys it is approximately 1–8%. Most cases still occur with no family history.
Can we wait until he is older to decide? Best not. The 6–18-month window has the best outcomes — both surgically and psychologically.
When to See a Pediatric Urologist
Book a consultation as soon as hypospadias is suspected — ideally in the first few weeks of life. The first visit will:
- Confirm the diagnosis and grade the severity
- Cancel any planned circumcision
- Check both testicles and the scrotum
- Plan the timing of surgery (usually 6–12 months)
For mild distal hypospadias, the road ahead is short and the outlook excellent. For more severe forms, the road is longer — but the destination of a normal-looking, normal-functioning penis is well within reach with expert care.
Dr. Tanmay Motiwala is an AIIMS-trained pediatric surgeon and pediatric urologist practising in Raipur, Chhattisgarh. He performs single-stage and two-stage hypospadias repair, with attention to cosmetic and functional outcomes. To book a consultation, visit the Contact page or call the clinic directly.
Related reading: Undescended Testis in Children | Phimosis in Boys: When Does Tight Foreskin Actually Need Treatment? | Preparing Your Child for Surgery
Sources: Hadidi — Hypospadias Surgery; Coran’s Pediatric Surgery (7th ed); Kelalis-King-Belman Clinical Pediatric Urology; Rob & Smith Operative Pediatric Surgery (7th ed).
📋 This article is part of Dr. Motiwala’s Pediatric Urology in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
- Undescended testis in baby boys
- Phimosis (tight foreskin) in boys
- Recurrent urine infections & hidden kidney problems
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is for educational and awareness purposes only. It is not a substitute for medical advice, diagnosis, or treatment, and is not a clinical consultation. Every child is different. If your child has any of the symptoms discussed, please consult your nearest qualified pediatric surgeon in person. In an emergency, go to the nearest hospital immediately.