“Doctor, the dentist says my baby has tongue-tie and needs to be cut. But she is feeding fine and gaining weight. Do we really need to do this?”
This is one of the most common worries I hear in my pediatric surgery clinic in Raipur. Tongue-tie is being diagnosed in a lot of babies these days — and many are pushed into a procedure they may not actually need. Here are the key things every parent should know.
What Is Tongue-Tie?
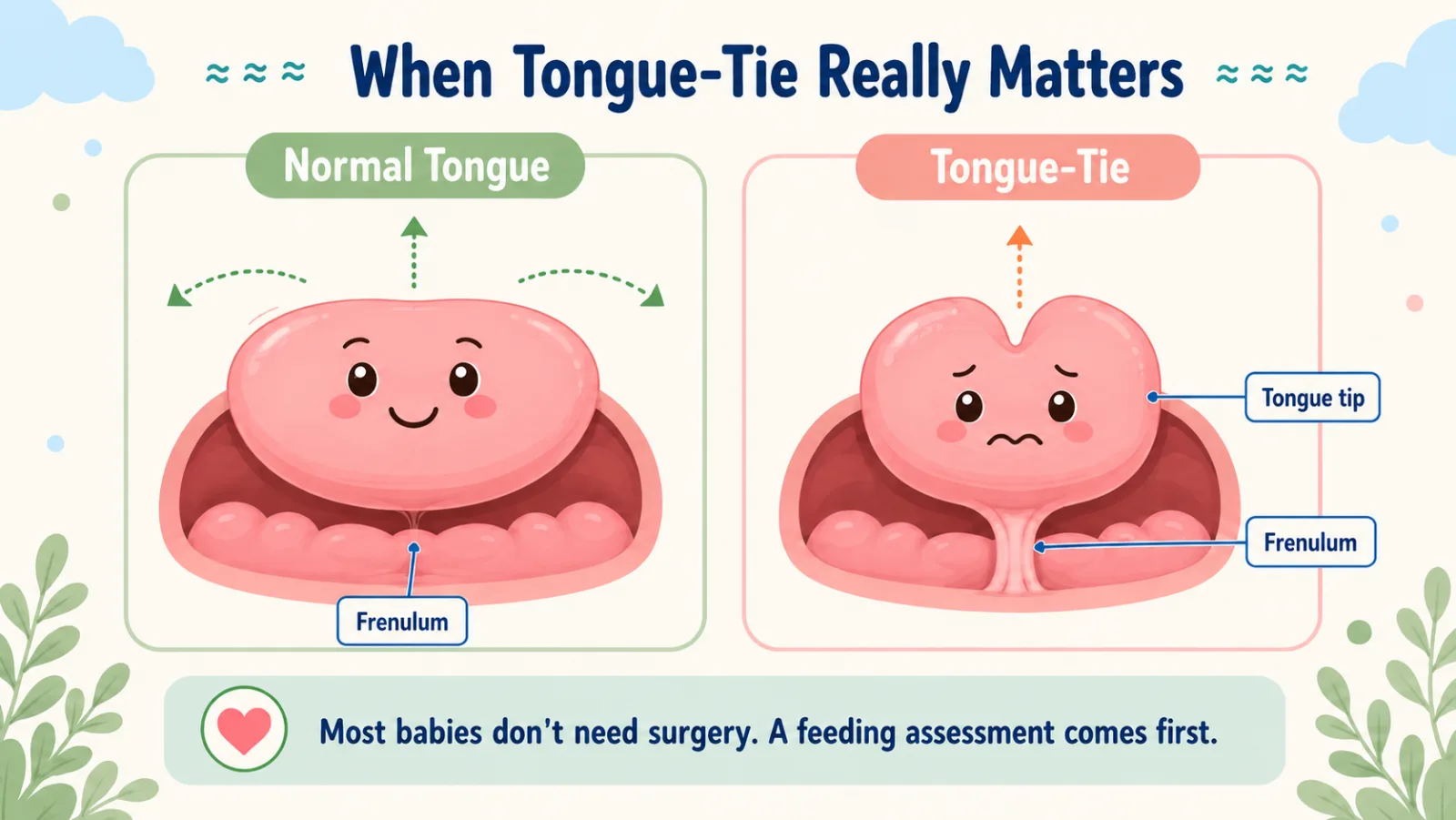
Under every baby’s tongue is a thin strip of tissue called the frenulum that connects the tongue to the floor of the mouth. In some babies this strip is short or attached too close to the tip — and that is tongue-tie, or ankyloglossia.
It is fairly common — found in about 5 to 10 out of 100 newborns, more often in boys. But here is the key point: being present is not the same as causing a problem.
When Does It Actually Matter?
In real practice, tongue-tie matters in only a few situations:
- Breastfeeding is genuinely failing — the baby cannot latch properly, the mother has cracked and painful nipples, and weight gain is poor.
- Older child has clear speech difficulty with sounds like t, d, l, r — and the tongue is visibly very restricted.
- The tongue cannot reach the lower teeth, leading to dental problems later.
If your baby is feeding well and gaining weight, a “tongue-tie” on a routine exam does not mean surgery is needed.
The Right Question to Ask
Not “does my baby have a frenulum?” — every baby does.
The right question is: “Is this baby feeding poorly because of the frenulum?”
Answering this properly needs a feeding assessment — by a lactation consultant or a pediatric surgeon — before anyone reaches for scissors or a laser.
The Procedure
If a release is genuinely needed, the operation is small:
- In newborns and young infants — a quick snip with sharp scissors in the clinic. The frenulum is thin and almost bloodless at this age. The baby cries for under a minute and goes straight back to the breast. No stitches, no anaesthesia.
- In older children — the frenulum is thicker and has blood vessels, so we do it as a short day-care procedure under general anaesthesia. The child goes home the same day.
That’s it. Done well, it is one of the simplest operations in pediatric surgery.
Things You May Have Heard — That Aren’t Quite Right
“Every baby with a frenulum needs it cut.”
No. Every baby has a frenulum. Most are completely fine.
“Laser is better than scissors.”
Studies show no difference in feeding outcomes between laser and scissors. Scissors are faster, cheaper, and safe.
“If we don’t cut it early, my child won’t speak properly.”
Most children with mild tongue-tie speak normally. Even if release is needed, doing it at age 2–3 works perfectly well.
“Tongue-tie causes colic, reflux, and poor sleep.”
There is no good evidence for this. Be careful of any clinic that blames a long list of unrelated problems on the tongue.
“You must do painful tongue stretches for weeks after the release.”
The evidence for this is very weak. Most pediatric surgeons advise *against* aggressive stretching, because it can cause the baby to refuse feeds altogether. Normal feeding and play allow the tongue to move plenty.
Common Questions Parents Ask
My baby’s tongue looks heart-shaped when she cries — is that bad? By itself, no. It just means the frenulum is there. If feeding and weight are fine, no action is needed.
Will my baby bleed a lot? In a newborn clinic frenotomy — usually a drop or two. In older children done under anaesthesia, bleeding is minimal and controlled.
Will it grow back? True reattachment is uncommon if the release was complete.
Can a dentist do this? The procedure itself is simple. What matters more than the tool is the diagnosis. Make sure a proper feeding assessment is done first.
When to See a Pediatric Surgeon
Book a consultation if:
- Your baby is not latching despite a lactation consultant’s help, and the tongue clearly looks tied
- Your baby is not gaining weight and you have been told it is “the tongue”
- Your nipples are cracked and bleeding and feeding has become unsustainable
- Your older child has clear speech difficulty with a visibly restricted tongue
- You want a second opinion before agreeing to a release suggested elsewhere
For a mild tongue-tie in a baby who is feeding and growing well, the textbook answer is the same as for many things in pediatric surgery: observe, reassure, and do not operate just because you can.
Dr. Tanmay Motiwala is an AIIMS-trained pediatric surgeon and pediatric urologist practising in Raipur, Chhattisgarh. He performs newborn frenotomy and frenuloplasty, after a careful feeding and functional assessment. To book a consultation, visit the Contact page or call the clinic directly.
Related reading: Preparing Your Child for Surgery — A Parent’s Guide | Is Surgery Safe for My Child?
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); DK Gupta Pediatric Surgery Vol 1.
📋 This article is part of Dr. Motiwala’s Neonatal & Newborn Surgery in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
- How to prepare your child for surgery
- Common pediatric surgical conditions every parent should know
- Is surgery safe for my child? 7 questions parents ask
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is for educational and awareness purposes only. It is not a substitute for medical advice, diagnosis, or treatment, and is not a clinical consultation. Every child is different. If your child has any of the symptoms discussed, please consult your nearest qualified pediatric surgeon in person. In an emergency, go to the nearest hospital immediately.