You have just fed your baby. Within minutes — before you have even put the burping cloth down — the milk comes shooting out, hitting the wall across the room. Your baby seems fine for a moment, then roots for the breast again as if nothing happened. This cycle repeats after every single feed. You have tried changing positions, burping more often, and feeding smaller amounts. Nothing works.
If this sounds familiar, it may not be ordinary reflux. It may be pyloric stenosis — a condition where the outlet of the stomach gradually blocks up in the first weeks of life.
It is easily treatable. But it needs to be found and fixed before your baby becomes seriously unwell.
What Is Pyloric Stenosis?
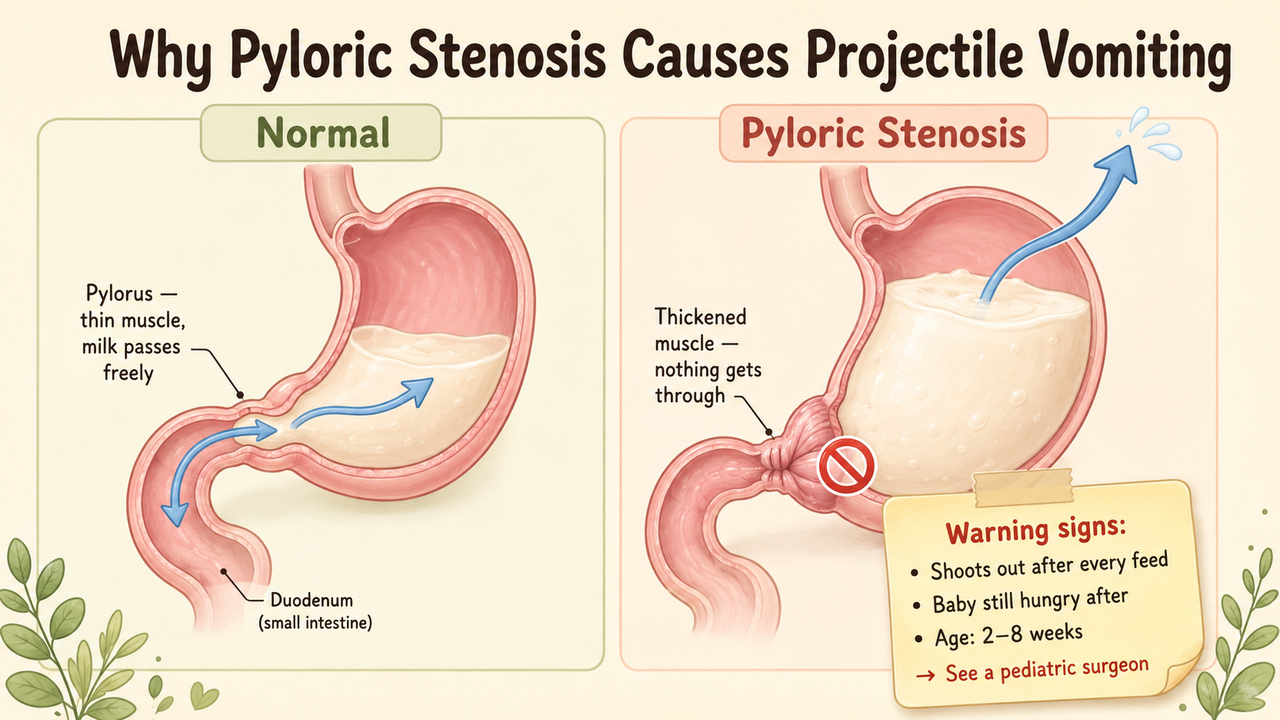
Between the stomach and the first part of the small intestine (the duodenum), there is a muscular valve called the pylorus. Its job is to open and let digested milk pass through in small amounts.
In a baby with pyloric stenosis, the muscle of this valve becomes progressively thicker and tighter over the first few weeks of life. The opening becomes so narrow that milk cannot get through properly. The stomach has nowhere to send the milk except back up — forcefully.
This is not the parents’ fault. It is not caused by anything you did during pregnancy or after birth. The muscle grows abnormally on its own, usually from about 2 to 3 weeks of age.
How Common Is It?
About 1.5 to 3 babies per 1,000 live births are affected — it is one of the most common reasons a young infant needs surgery.
It is four times more common in boys than in girls. It is most common in first-born males. If a parent had pyloric stenosis as an infant, the baby’s risk is somewhat higher.
What Does It Look Like?
The key features that point to pyloric stenosis — and not ordinary reflux — are:
The vomiting is projectile. The milk shoots out with force, often landing far from the baby. This is very different from the normal posseting (gentle spilling) of reflux.
The vomiting is non-bilious. The vomit is milk-coloured or curdled white. It should never be yellow or green. If it is, that means something different is happening and you should go to a hospital immediately.
The baby is hungry again immediately after vomiting. They did not vomit because they were full or unwell — they vomit because the stomach could not empty. They are still hungry.
The timing. Symptoms usually appear between 2 and 8 weeks of age, with a peak at 3 to 5 weeks. A baby who vomits like this from birth, or for the first time at 3 or 4 months, is less likely to have pyloric stenosis.
Weight loss or poor weight gain. Because the baby cannot keep milk down, they are not absorbing enough nutrition. They may look thin, hungry, and irritable.
How Will the Doctor Know?
When an experienced doctor examines a baby with pyloric stenosis, they can sometimes feel the thickened pylorus muscle directly — it feels like a small, smooth, firm olive-shaped lump in the upper abdomen. This is called the “pyloric olive.”
The diagnosis is confirmed by a simple ultrasound scan. The radiologist measures the thickness of the pyloric muscle (normal is under 3 mm; in pyloric stenosis it is 4 mm or more) and the length of the narrowed channel (16 mm or longer). The ultrasound is accurate, takes only a few minutes, and involves no radiation.
Why Is It Not Just Reflux?
Ordinary gastro-oesophageal reflux (the most common reason babies vomit) is different:
| | Pyloric Stenosis | Reflux | |—|—|—| | Vomiting force | Projectile — shoots out | Gentle spill or posset | | Bile | Never (white/creamy) | Never (white/creamy) | | Baby after vomiting | Immediately hungry | Usually contented | | Age of onset | 2–8 weeks | From birth | | Weight gain | Failing or dropping | Usually normal |
If the vomiting is projectile and the baby always looks hungry after, see a pediatric surgeon — not just a general practitioner — for an ultrasound.
What Needs to Happen Before Surgery?
This is one of the most important things for parents to understand: pyloric stenosis is a medical emergency first, not a surgical one.
By the time a baby is brought to hospital, they may have lost significant fluids and salts from all the vomiting. This causes a specific blood chemistry imbalance — a condition called hypochloremic hypokalemic metabolic alkalosis — which means the blood has too little chloride and too little potassium, and it has become too alkaline.
Performing surgery on a baby with severely abnormal blood chemistry is dangerous. So the first step is always to:
- Put up an intravenous line
- Give fluid and electrolyte replacement over 12–48 hours
- Check the blood chemistry repeatedly until it has corrected
Only then is it safe to operate. Do not be alarmed if the surgery is not done on the day of admission — this delay is deliberate and protects your baby.
What Is the Surgery?
The operation is called a Ramstedt pyloromyotomy. It is one of the most elegant and reliable operations in pediatric surgery.
Under general anaesthesia, the surgeon makes a small incision — today almost always laparoscopically through 3 tiny holes. The thickened pyloric muscle is carefully split along its length, from the outer layer all the way down to the lining inside — but without cutting that inner lining. When the muscle is divided this way, the two halves spring open, and the narrowed channel immediately opens up wide.
The inner lining bulges out gently into the gap — which is exactly what is supposed to happen. The stomach can now empty normally.
The operation takes 30–45 minutes. Your baby wakes up in the recovery room, usually comfortable.
What Happens After Surgery?
Feeding is started gently — usually with small amounts of expressed breast milk or formula — 4 to 6 hours after surgery. Volumes are increased gradually over the next 24 hours.
A little vomiting on the day after surgery is completely normal — the stomach has been stretched for weeks and needs a day or two to calm down. It is not a sign that the operation has failed.
Most babies go home within 24 to 48 hours of surgery.
The outcome of this operation is excellent — essentially a complete cure. Long-term studies show no difference in gastric emptying or digestive function between adults who had a pyloromyotomy as infants and those who never had the condition.
What to Watch For at Home
See a doctor immediately if your baby:
- Continues to vomit forcefully after feeds beyond the second day after surgery
- Passes green or yellow vomit at any time
- Becomes lethargic, pale, or very difficult to rouse
- Develops redness or swelling around the small wound
These are uncommon but warrant immediate review.
When to See a Pediatric Surgeon
Come to a paediatric surgical centre without delay if:
- Your baby (aged 2–10 weeks) is vomiting powerfully after every feed
- The vomiting has been getting progressively worse over days
- Your baby looks hungry and unsatisfied after vomiting
- Your baby is not gaining weight or is losing weight
Do not wait several days hoping it will pass. The earlier pyloric stenosis is diagnosed, the less dehydrated and unwell your baby will be — and the quicker the recovery.
https://www.youtube.com/watch?v=placeholder
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He manages infants with pyloric stenosis and other surgical conditions of the stomach and bowel. To book a consultation, visit the Contact page or call the clinic directly.
📋 This article is part of Dr. Motiwala’s Pediatric General & Abdominal Surgery in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
- Intussusception (sudden tummy pain + blood in stool)
- Biliary atresia (newborn jaundice that won’t clear)
- Hirschsprung disease
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child. In an emergency, go to the nearest hospital immediately.
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); DK Gupta Pediatric Surgery Vol 1.