
If your newborn baby has been told they have an anorectal malformation — or that the bottom opening is not formed properly — I know that is a frightening thing to hear, especially in the first hours after birth.
I want to explain it to you in simple words. No complicated terms. Just what it is, what we do about it, and what your child’s life will look like.
What Exactly Is Wrong?
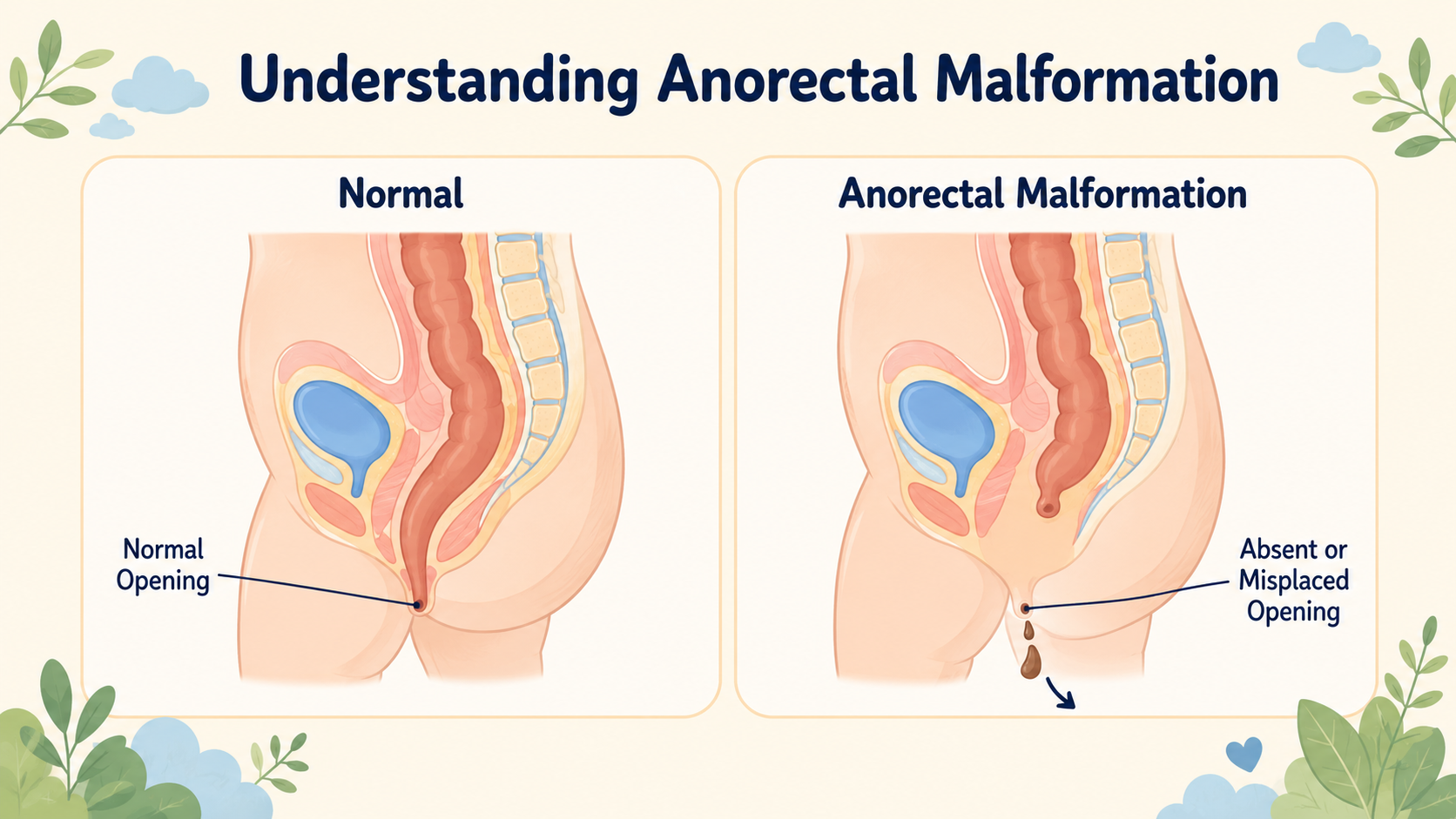
Before a baby is born, the lower part of the gut needs to form properly — including the opening at the bottom where stool comes out. In some babies, this does not form the way it should. The opening may be completely absent, very small, or in the wrong place.
This is called an anorectal malformation — which just means “the bottom end of the bowel did not form normally.”
This is nobody’s fault. It is not something you did during pregnancy. It happens during the very early weeks of development in the womb, before most mothers even know they are pregnant.
How Is It Found?
In most cases, the nurse or doctor who checks the baby at birth will notice it straightaway. They look at every newborn baby’s bottom as part of the routine check. Sometimes the opening is missing. Sometimes the baby passes the first black stool (called meconium) from an unusual place — near the scrotum in boys, or near the vagina in girls. That is the first sign.
Will My Baby Be Okay?
Yes — but it will need surgery. The good news is that this is a known, treatable condition. Surgeons who specialize in children have been doing this surgery for decades, and most children do very well.
What Happens First?
The first thing we do is not rush. We wait about 24 hours so we can understand exactly what type of problem the baby has. Not all anorectal malformations are the same — some are simpler, some are more complex — and the type decides the next step.
If it is a simpler type: We may be able to do a repair directly in the first few days of life. One surgery, and the baby goes home with a normally positioned opening.
If it is a more complex type: We do a smaller first surgery to give the baby a temporary opening in the tummy (called a colostomy). Through this opening, stool comes out into a small bag on the outside. This keeps the baby comfortable and growing while we plan the main surgery. The bag is temporary — it is not permanent.
What Is the Main Surgery?
The main surgery is called a PSARP — but you don’t need to remember that name. In simple terms: the surgeon opens the back area, finds the bowel, and moves it to the right position — exactly in the centre of the bottom muscle. This muscle is what will eventually control the stool.
The baby is face-down during the surgery. The surgeon uses a small device that beeps near muscle tissue, so they can find the exact centre and make sure the bowel is placed in the right spot.
This surgery is usually done when the baby is about 3 to 6 months old and has grown a little bigger.
What Do We Do After Surgery?
After the main surgery, we teach the parents to do something called dilatations at home. This just means gently passing a small smooth plastic stick into the new opening, twice a day, to make sure it does not become tight as it heals. We show you exactly how to do it in the clinic. It looks scary at first, but most parents manage it comfortably within a week.
Once the opening has healed well and reached the right size, we close the tummy opening (the colostomy) in a third small surgery. After that, the baby has one normal opening, in the right place, just like any other child.
Will My Child Be Able to Pass Stool Normally?
This is the question every family asks, and I want to give you an honest answer — not a reassuring one.
It depends on the type of malformation. The outlook is very different for simpler versus more complex cases.
For children with a simpler (low) type — where the bowel came close to the skin surface — around 80 to 90% achieve full stool control over time. This is genuinely good news.
For children with a more complex (high) type — where the bowel ended near the bladder or urethra — the numbers are more difficult. Studies show that only about 1 in 5 to 1 in 3 of these children achieve full independent stool control. The rest need ongoing help.
That help comes in the form of a daily bowel wash-out routine — a small amount of water is gently put into the back passage once a day at a set time, which empties the bowel completely. After that, the child stays clean for the rest of the day and can go to school, play, and live normally without accidents. It is not a cure for the underlying problem, but it gives the child a normal daily life. Many children and their families manage this very well with the right training.
What decides the outcome more than anything else is something called the sacrum — the bone at the base of the spine. If this bone is poorly formed, the nerves in the area are limited from the start, and no surgery can fully overcome that. We look at this on an X-ray before the operation and counsel families honestly based on what we see.
The most common problem after surgery — even in children doing well — is constipation. The bowel above the repair tends to be slow. This needs active management with medicines and diet, and should not be left unaddressed.
Long-term follow-up with the surgeon matters for all children with this condition, not just those who are struggling.
Does My Child Have Any Other Problems to Watch For?
Studies show 50 to 70 percent of babies with this condition have one or more other issues — with the kidneys, spine, or heart — that are also present from birth. So after the baby is stabilized, we do a few routine scans: kidney ultrasound, spine ultrasound, and a heart check. These are done to make sure nothing is missed, not because we expect something serious. Many babies have no other issues at all.
The Most Important Thing to Know
Your baby needs surgery — but this is not an emergency that needs to happen in the next hour. It needs to happen in the right order, with the right preparation, at a centre that does these operations regularly.
If you have been told your baby has this condition and you are in Chhattisgarh or a nearby area, bring the baby to a paediatric surgical centre as soon as you can so we can assess exactly what type it is and make a plan.
📋 This article is part of Dr. Motiwala’s Pediatric Colorectal & Anorectal Surgery in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child.
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He sees children with complex bowel conditions from across Chhattisgarh and central India. To book a consultation, visit the Contact page.
Related reading:
- Baby Not Passing Stool? It Could Be Hirschsprung Disease
- My Child Has a Swelling in the Groin — Is It a Hernia?
- Is Surgery Safe for My Child?
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); Peña — Colorectal Surgery in Children; Holschneider — Anorectal Malformations (2nd ed).



One Response
The way this article has explained about the rare abnomrality with a calm tone is impressive as it reduce the fear and improve the confidence in the readers. Great job.