Every healthy newborn baby should pass their first black, sticky stool — called meconium — within the first 24 to 48 hours of life. If your baby has not passed any stool for more than 2 days, and their tummy is looking swollen, that is something a doctor needs to check.
One condition I look for in this situation is called Hirschsprung disease. It sounds like a difficult name, but the idea behind it is simple — and so is the answer once we confirm it.
What Is Hirschsprung Disease?
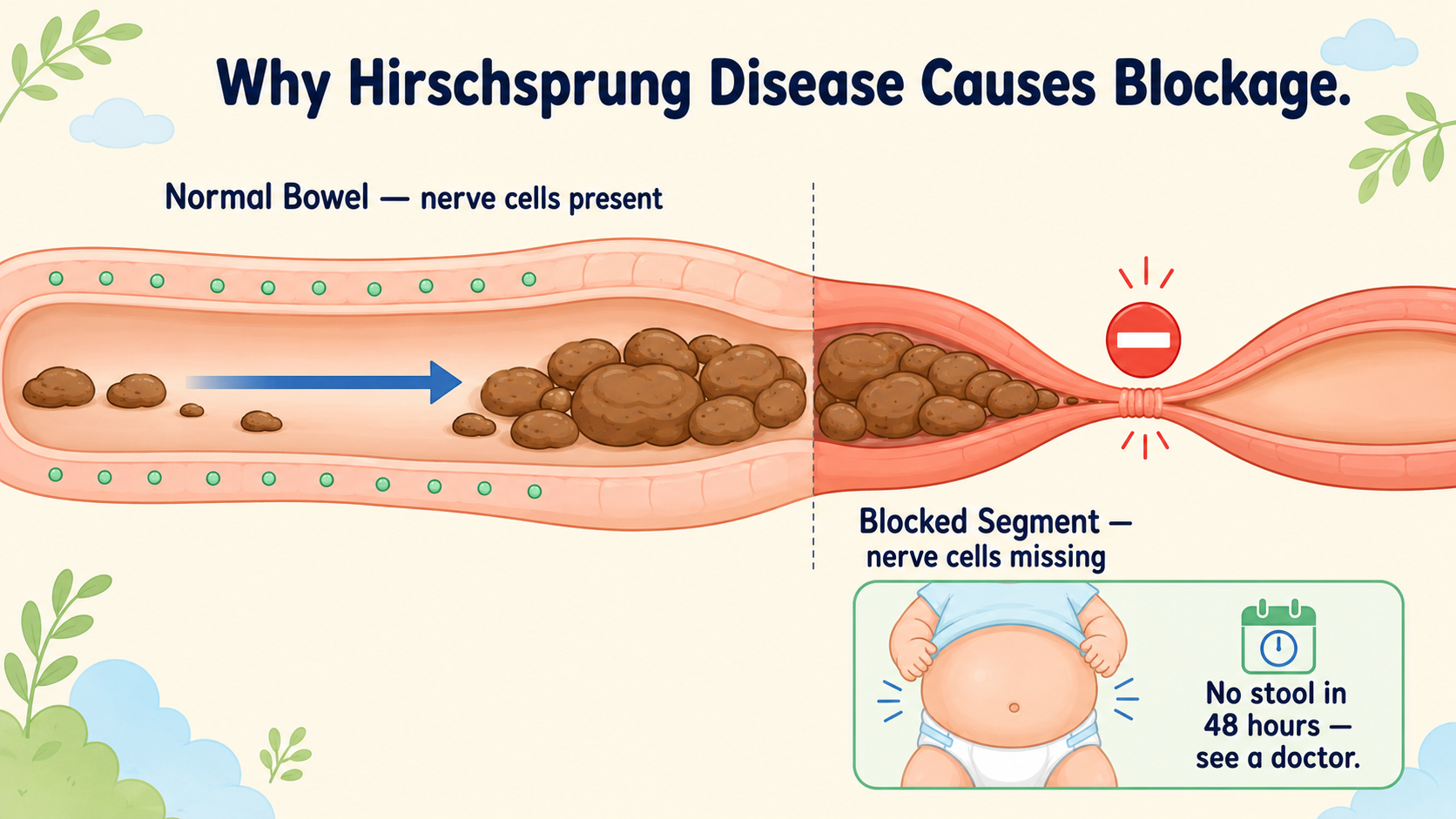
Think of the bowel like a long tube. For stool to move through it and come out, the bowel wall needs to squeeze and push — like how you squeeze a tube of toothpaste from one end to the other.
For this squeezing to happen, there are tiny nerve cells inside the bowel wall that send the signal to squeeze. In a baby with Hirschsprung disease, these nerve cells are missing from the lower part of the bowel. The signal never arrives. That part of the bowel stays stiff and tight — like a blocked pipe — and stool cannot get through. This is not the parents’ fault. It happens during the baby’s development in the womb, before birth.
How Do I Know If My Baby Has This?
The most common sign in a newborn is simple: no stool in the first 48 hours, with a swollen, tight-looking tummy.
In slightly older babies, the signs look different. These babies have had trouble passing stool since the very beginning — from the first weeks of life. Their tummy is always a little bloated. Normal dietary changes or simple medicines do not help. Sometimes they pass a sudden large burst of very watery stool after going many days without anything — this is not diarrhoea, it is stool leaking around a blockage.
The key difference from ordinary constipation: ordinary constipation in babies does not start from day one of life, and it usually gets better with small changes. Hirschsprung disease does not.
How Does the Doctor Confirm It?
An X-ray with a dye: A small amount of safe dye is placed gently into the back passage. On the X-ray, we can see where the narrow, blocked part of the bowel ends and where the normal, wider bowel begins. This tells us how much of the bowel is affected.
A small tissue test (biopsy): A tiny piece of tissue — smaller than a grain of rice — is taken from just inside the back passage. No operation needed for this; it takes a few minutes. A lab then checks whether the nerve cells are present or absent. This is the most reliable way to confirm the diagnosis.
What Is the Treatment?
The treatment is surgery. There is no medicine that can replace the missing nerve cells. The surgery removes the part of the bowel that has no nerve cells and joins the healthy bowel down to just above the bottom opening, so stool can pass normally.
For most babies with the common type, this is done as a single surgery through the bottom passage itself. The child does not need a permanent bag.
In some cases — if the baby is very unwell when they arrive, or the blockage has been there a long time — we first put a small temporary opening in the tummy to let stool out safely. This is always temporary and is closed later once the baby has recovered.
What Happens After Surgery?
In the first few months after surgery, the baby will pass stool frequently and it will be loose. This is completely normal — the bowel is adjusting. It usually improves within 6 to 9 months.
After surgery, we teach parents to gently pass a small smooth stick into the bottom opening twice a day. This keeps the opening from becoming too tight as it heals. Most parents manage it well once shown.
About long-term bowel function — an honest picture:
Most children improve steadily through childhood. Puberty is when the final improvement usually happens, not necessarily school age. Many children by their mid-teens report a good quality of life and are functioning normally day to day.
However, the numbers are worth knowing. Studies show that 10 to 30% of children have some ongoing soiling after surgery. Some develop constipation again — because the internal muscle at the bottom can stay tighter than normal even after a technically good operation. This often improves with a simple procedure (an injection to relax the muscle), but it may need attention more than once.
Even in adults who have had a good outcome, research shows that bowel function scores remain lower than in people who never had the condition. Some adults find that their control slowly gets more difficult as they get older, which is why long-term follow-up with a surgeon matters.
The point is not to alarm you. Most children live full, normal lives. But this is a condition that needs honest monitoring and follow-up — not just surgery and discharge.
One Warning That Every Parent Must Know
Sometimes, a child with Hirschsprung disease — before or after surgery — can develop a serious infection in the bowel. The signs are:
- Sudden, very watery and foul-smelling stool
- A very swollen, hard tummy
- Fever
- The baby looks very unwell — pale, not feeding, very sleepy
If you see these signs, go to a hospital immediately. Do not wait. This is a medical emergency that needs treatment within hours.
When Should I See a Pediatric Surgeon?
Come to a paediatric surgical centre without delay if:
- Your newborn has not passed any stool in 48 hours and the tummy looks swollen
- Your baby has had difficulty passing stool since the very first weeks of life
- Your baby’s tummy always looks bloated, even after passing stool
- A child with known Hirschsprung disease suddenly develops a swollen tummy, watery stool, and fever
📋 This article is part of Dr. Motiwala’s Pediatric Colorectal & Anorectal Surgery in Raipur services — see the full range of conditions treated, what to expect, and when to see a pediatric surgeon.
Related conditions parents also read
- Anorectal malformation (born without a normal anal opening)
- Constipation in children
- Pyloric stenosis (forceful vomiting in babies)
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child.
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He treats newborns and children with bowel conditions from across Chhattisgarh and central India. To book a consultation, visit the Contact page.
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); DK Gupta Pediatric Surgery Vol 1.