Most newborns turn a little yellow in the first week of life. Usually it is harmless and fades on its own. But sometimes the yellow does not go away — and a small number of these babies have a serious, hidden problem with the liver that is silently getting worse every week.
There is one rule every parent and doctor should hold on to:
> Any baby who is still jaundiced (yellow) after 2 weeks of age must have a blood test to check the type of bilirubin — without delay.
That single test can be the difference between saving a baby’s own liver and needing a liver transplant. This article explains why.
Two Very Different Kinds of Newborn Jaundice
Jaundice means a yellow colour of the skin and the whites of the eyes, caused by a pigment called bilirubin building up in the blood. There are two completely different types, and they are not the same problem at all:
- “Indirect” (unconjugated) jaundice — the common, usually harmless kind. It appears in the first days of life (physiological jaundice or breast-milk jaundice) and almost always settles by itself.
- “Direct” (conjugated) jaundice — the dangerous kind. Here the liver makes bilirubin ready to leave the body, but it cannot get out because the drainage pipes (bile ducts) are blocked. This type is never normal in a baby, at any age.
A simple blood test — a fractionated or split bilirubin — tells the two apart. This is why a baby still yellow at 2 weeks must be tested, not just reassured.
The Condition We Are Most Afraid of: Biliary Atresia
The most important cause of dangerous (conjugated) jaundice in a young baby is biliary atresia.
In biliary atresia, the bile ducts — the tiny pipes that carry bile from the liver to the intestine — become inflamed, scarred, and blocked, usually in the first weeks of life. Bile cannot drain, so it backs up and damages the liver. Left untreated, this leads to scarring of the liver (cirrhosis) and, eventually, liver failure.
It is not common — it affects roughly 1 in 10,000 to 1 in 18,000 babies — and it is somewhat more frequent in Asian countries. But it is the single most common reason a child ever needs a liver transplant, which is exactly why it must never be missed.
The Three Red Flags Parents Should Watch For
Biliary atresia hides inside an otherwise healthy-looking, feeding, growing baby. The warning signs are:
1. Jaundice that lasts beyond 2 weeks of age — the skin and the whites of the eyes stay yellow instead of clearing.
2. Pale, clay-coloured or chalky-white stools. This is the most important sign. When bile cannot reach the intestine, the stool loses its normal yellow-green colour and turns pale, putty-like or white. Early on the stools can look normal in up to half of babies, so this can develop gradually — keep checking the nappy colour.
3. Dark urine. A newborn’s urine should be almost colourless. Urine that is persistently dark yellow or brown — staining the nappy — is a warning sign, because the blocked bilirubin is being passed out through the kidneys instead.
A doctor may also feel that the liver is enlarged and firm. If you ever see pale stools and dark urine together in a young baby, treat it as urgent.
Why the Timing of Surgery Is Everything
Biliary atresia is treated with an operation called the Kasai procedure (hepatic portoenterostomy). The surgeon removes the scarred, blocked ducts and connects a loop of intestine directly to the surface of the liver, so that bile can drain again.
The Kasai operation is not a cure — it is a way to restore bile flow and protect the baby’s own liver for as long as possible. And here is the crucial part: it works far better the earlier it is done, before the liver is badly scarred.
For many years the teaching was a strict deadline of 60 days of age. We now understand the picture is a little more forgiving than that — for typical biliary atresia, the chance of clearing the jaundice holds up reasonably well until around 8 to 12 weeks, after which outcomes clearly worsen. But the liver is scarring a little more every single week. So the goal has not really changed: diagnose early and operate as early as possible — ideally well before 3 months of age. A baby diagnosed at 3 weeks does far better than one diagnosed at 3 months.
This is the entire reason for the 2-week rule. A delay of a few weeks in testing a yellow baby can be the difference between a working liver and a transplant.
What Happens After a Kasai Operation — The Honest Picture
Parents deserve a truthful picture so they can plan, not false comfort.
- After a Kasai, bile starts draining in about two-thirds of babies, and the jaundice fully clears in roughly 55–60%.
- Even when the operation goes well, the underlying liver disease often keeps progressing. Over time, about 70–80% of children with biliary atresia eventually need a liver transplant — for many, the Kasai buys precious years of growth first.
- Survival with the child’s own (native) liver is roughly 45–50% at 5 years, falling to around 30–45% at 10 years. Some children do reach adulthood with their own liver, but they usually need careful lifelong follow-up.
None of this is meant to frighten — it is meant to explain why early diagnosis matters so much. A baby operated on early, before the liver is heavily scarred, has the best possible chance in every one of these numbers. Children who reach transplant today also have excellent long-term outcomes.
What Every Parent Must Know
- A little yellow in the first week is usually normal.
- Jaundice that is still there at 2 weeks is not something to “wait and watch” — it needs a blood test for the type of bilirubin.
- Pale/white stools + dark urine in a baby is a red flag — seek review the same day.
- Biliary atresia is treatable, and the result depends heavily on how early it is found.
If you are ever told your jaundiced baby is “fine, it’s just breast-milk jaundice” but the stools look pale, ask specifically for a split (conjugated) bilirubin test. It is a simple test, and it is the one that protects the liver.
When to See a Pediatric Surgeon
Any baby with jaundice persisting beyond 2 weeks — and especially any baby with pale stools and dark urine — should be evaluated promptly. A raised conjugated bilirubin needs urgent assessment at a centre with paediatric surgical and liver expertise, because the workup and any Kasai surgery are time-sensitive.
Dr. Tanmay Motiwala is a pediatric surgeon in Raipur, Chhattisgarh, trained at AIIMS Jodhpur. He evaluates and manages newborns with prolonged jaundice and suspected biliary atresia from across Chhattisgarh and central India. If your baby is still yellow at 2 weeks of age, do not wait — ask your doctor for a conjugated bilirubin test.
Related reading:
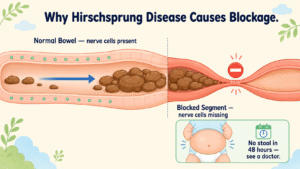
- Baby Not Passing Stool Since Birth? It Could Be Hirschsprung Disease
- My Baby Was Born Without a Normal Bottom Opening — Understanding Anorectal Malformation
- Common Pediatric Surgical Conditions Every Parent Should Know
⚠️ Important Disclaimer: This article is for general information and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Every child’s condition is different — facts, prognosis, and management can vary significantly from case to case. Please consult a qualified pediatric surgeon for advice specific to your child.
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed).