A bulging belly button in a baby is one of the most common worries that brings parents to my pediatric surgery clinic in Raipur. The good news is simple: in almost every baby, an umbilical hernia closes on its own without any treatment.
The bad news is that there is a lot of well-meant but unhelpful advice — coins taped over the navel, tight belly binders, special oils — none of which actually work. Here is what parents really need to know.
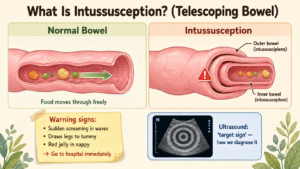
What Is an Umbilical Hernia?
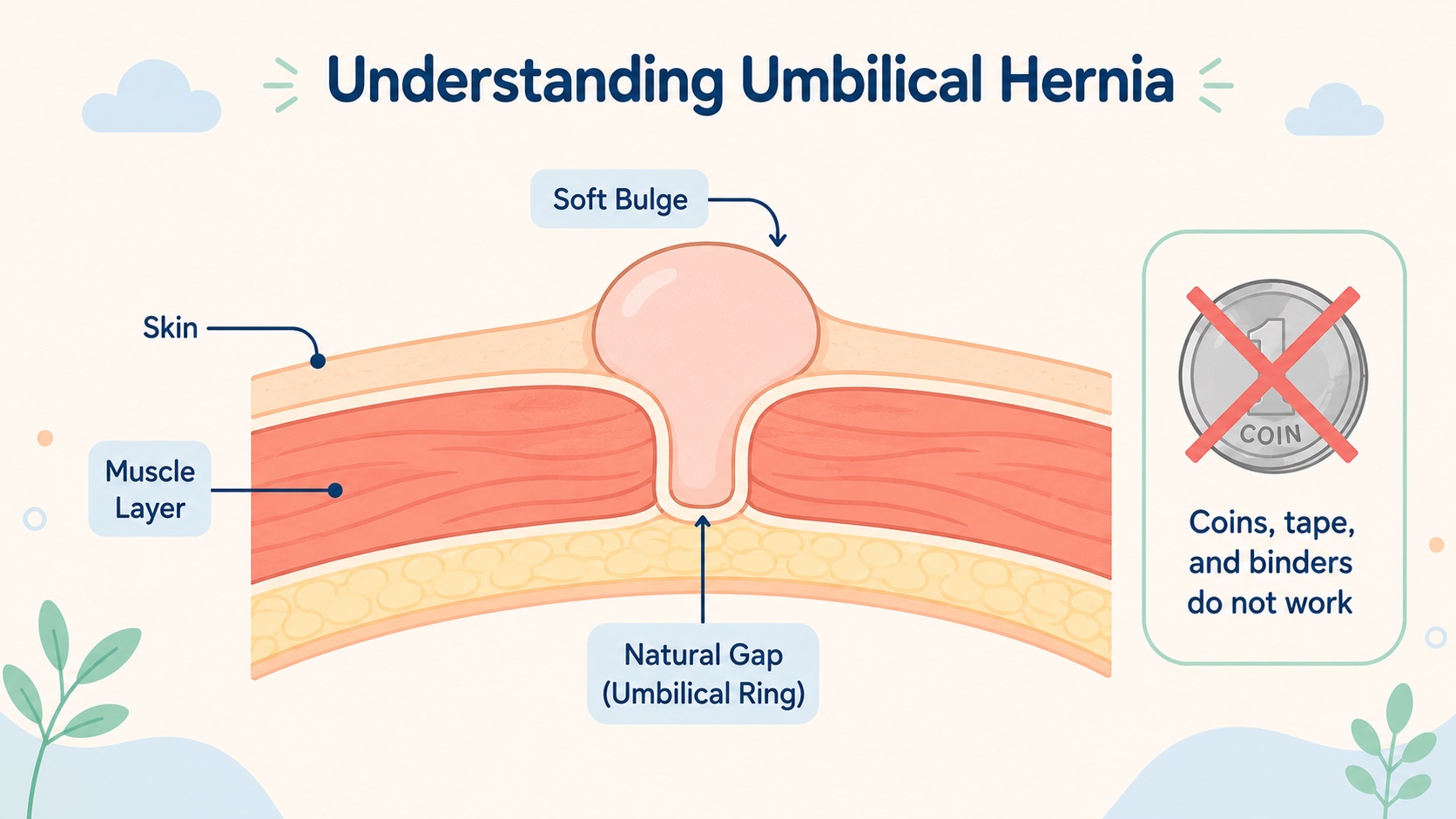
Before birth, the umbilical cord passes through a natural gap in your baby’s tummy wall, at the navel. After birth, this gap is supposed to close as the muscle grows together. In some babies, the gap stays open for a while. A little bit of intestine, covered by skin, pushes out through the gap — and that’s the soft bulge you see.
It is not the same as a groin hernia. An umbilical hernia in a baby is far less risky.
How Common Is It?
Very common — found in about 1 in 5 full-term newborns (about 20%). It is even more common in:
- Premature babies — up to 75–80% of small premature babies have one.
- Babies of African descent.
- Babies with certain conditions like Down syndrome or hypothyroidism.
It happens equally in boys and girls.
Will It Close on Its Own?
Yes — almost always. This is the most important fact for parents.
Unlike a groin hernia, the muscle ring at the navel keeps closing for months and even years after birth. About 80% of umbilical hernias close on their own by 3 to 5 years of age. No medicines, no surgery, no special tricks — just time.
The chance of natural closure depends on the size of the gap in the muscle, not how big the bulge looks. A small gap (under 1.5 cm across) almost always closes by itself. A larger gap may not.
Is There a Risk of It Getting Stuck?
This is what most parents fear, and the truth is reassuring:
- The risk of an umbilical hernia getting strangled is about 1 in 1,500 — very, very rare.
- This is far less risky than a groin hernia, which is why the two are treated very differently.
So unless the bulge becomes suddenly hard, painful, red, or refuses to push back in, there is no urgency.
The Coin, the Tape, the Belly Binder — Please Don’t
In many Indian homes, well-meaning relatives suggest pressing a coin or button over the navel and taping it down, or wrapping a tight cloth around the tummy. Some say this will “push the hernia in” or “speed up healing.”
Please do not do this. Every modern pediatric surgery textbook lists these as discredited practices. They:
- Do not close the muscle gap any faster.
- Can cause skin rashes, sores, and infection under the tape.
- Sometimes lead to an infection that itself needs treatment.
- Give a false sense of “doing something” while the real answer is simply to wait.
The right approach is observation, reassurance, and follow-up. Nothing more.
When Is Surgery Needed?
Surgery is reserved for specific situations:
- The hernia is still there at 4–5 years of age. This is the standard age cutoff used worldwide.
- The muscle gap is large — typically more than 1.5–2 cm. Large gaps rarely close on their own.
- The hernia is long and trunk-like (“proboscoid”) and clearly not getting smaller — may be repaired earlier.
- Complications occur — sudden pain, hardness, redness, or non-reducibility. These are emergencies.
If your child is under 4 and the hernia is small, soft, and painless, the right thing to do is wait. There is no advantage to operating early.
What Is the Surgery Like?
It is one of the simpler operations in pediatric surgery and is done as a day-care procedure.
- A small curved cut (under 2 cm) is made just below the belly button, hidden in the natural crease.
- The hernia sac is opened and the contents are gently returned to the tummy.
- The muscle edges are stitched together with strong dissolving sutures.
- A special umbilicoplasty stitch is placed to recreate the natural “dimple” of the belly button — so the cosmetic result is excellent.
The operation takes about 30 minutes under general anaesthesia.
After Surgery
- Your child is discharged the same day.
- Mild discomfort for 24–48 hours is managed with paracetamol.
- Stitches dissolve on their own.
- Keep the wound dry for 3–4 days; sponge bath only during this time.
- Back to school in about a week, back to sports in 2–3 weeks.
- Infection or small blood collection happens in about 1% of cases.
- Recurrence is under 1%.
Common Questions Parents Ask
My baby’s belly button gets huge when she cries — is that bad? No. Crying just makes it more visible. It does not damage anything.
Should I avoid tummy-time or massage? No. Normal play and gentle massage make no difference.
Can I push it back in? Yes, a soft umbilical hernia pushes back easily. But there is no need to keep doing it. It will pop out again next time the baby cries — and that is fine.
Will surgery leave a scar? The scar is hidden inside the belly button and is essentially invisible.
My child is 6 and still has it — is it too late? No. Repair at this age is straightforward with excellent results.
When to See a Pediatric Surgeon
Book a consultation if:
- Your child has an umbilical hernia that has not closed by age 4.
- The gap feels large (you can fit a fingertip in easily).
- The hernia is painful, red, or tender — this is urgent.
- The bulge suddenly becomes hard and won’t push back in — go to the emergency room.
For everything else — a small, soft, painless belly-button bulge in a baby — the textbook answer is simply: wait, watch, and reassure.
Dr. Tanmay Motiwala is a pediatric surgeon practising in Raipur, Chhattisgarh. He performs day-care umbilical and inguinal hernia repairs in children of all ages, with attention to a neat cosmetic result. To book a consultation, visit the Contact page or call the clinic directly.
Related reading:
- My Child Has a Swelling Near the Groin — Could It Be a Hernia?
- Hydrocele in Baby Boys: Why the Scrotum Looks Swollen
Sources: Coran’s Pediatric Surgery (7th ed); Rob & Smith Operative Pediatric Surgery (7th ed); DK Gupta Pediatric Surgery Vol 1.
Related conditions parents also read
- Inguinal hernia in children (groin swelling)
- Common pediatric surgical conditions every parent should know
- Hydrocele in baby boys
Worried about your child? Dr. Tanmay Motiwala consults in Raipur, Jagdalpur & Rajim. Book an appointment or call +91 83190 84711.
⚠️ Important Disclaimer: This article is provided purely for educational and awareness purposes. The information here is not a substitute for medical advice, diagnosis, or treatment, and should not be considered as an OPD or clinical consultation. Every child is different — symptoms that look the same may have different causes. If your child has any of the conditions or symptoms discussed, please consult your nearest qualified pediatric surgeon in person for an examination and personalised advice. In an emergency, go to the nearest hospital immediately.